Increasing Vegetable Intakes Rationale and Systematic Review of Published Interventions
![]()
Global Vegetable Intake and Supply Compared to Recommendations: A Systematic Review
i
Segmentation of Human Diet and Health, Wageningen University, PO Box 17, 6700 AA Wageningen, Gelderland, Holland
2
Unilever Foods Innovation Eye, Bronland 14, 6708 WH Wageningen, Gelderland, The netherlands
*
Author to whom correspondence should be addressed.
Received: 3 May 2020 / Revised: 20 May 2020 / Accustomed: 21 May 2020 / Published: 27 May 2020
Abstract
Low vegetable intake is associated with higher incidence of noncommunicable diseases. Data on global vegetable intake excluding legumes and potatoes is currently lacking. A systematic review following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines was conducted to assess vegetable consumption and supply in adult populations and to compare these data to the existing recommendations (≥240 grand/twenty-four hour period according to World Health Organisation). For vegetable intake information online, websites of regime institutions and health authorities, European Food Safe Authority (EFSA) Comprehensive European Food Consumption Database, STEPwise arroyo to surveillance (STEPS) and Pubmed/Medline databases were searched from March 2018 to June 2019. Vegetable supply information was extracted from Nutrient Balance Sheets, Food and Agriculture Arrangement Corporate Statistical Database (FAOSTAT), 2013. Vegetable intake was expressed as means and 95% conviction intervals. Data were summarized for each region by calculating weighted means. Vegetable intake and supply data were available for 162 and 136 countries, respectively. Weighted mean vegetable intake was 186 g/twenty-four hours (56–349 yard/day). Weighted mean vegetable supply was 431 chiliad/24-hour interval (71–882 g/solar day). For 88% of the countries vegetable intake was below the recommendations. Public health campaigns are required to encourage vegetable consumption worldwide. In the 61% of the countries where vegetable supply is currently insufficient to run into the recommendations, innovative food organization approaches to ameliorate yields and decrease post-harvest losses are imperative.
1. Introduction
The incidence of chronic, noncommunicable diseases (NCDs) (mainly cardiovascular diseases (CVDs), cancer, chronic respiratory disease and diabetes) is increasing rapidly and is having a significant impact on society, economy and health [1,2,iii,4]. Currently, 70% of deaths are caused past NCDs worldwide [1]. A major take chances factor for NCDs is an unhealthy diet, including low vegetable consumption [iv,5].
Multiple studies indicated a positive relation between vegetable intake and reduction of CVDs [3,6,7,8,9,10,eleven,12,13,14,15,xvi,17,18]. In a meta-assay by Zhan et al. (2017) [18], the pooled relative take a chance (RR) for CVDs between highest versus lowest vegetable intake category was 0.87 (95% CI: 0.83–0.91), which indicates a decreased CVD adventure with increasing vegetable intake. Associations betwixt vegetable intake and adiposity [2,nineteen,20,21], type 2 diabetes [2,22,23,24,25,26,27,28,29], chronic respiratory diseases [thirty,31] and cancer [two,8,32,33,34,35,36,37,38] are less consistent. The benefits of vegetables on prevention of NCDs can exist explained by the relatively high content of micronutrients, antioxidant compounds, polyphenols and fibers in vegetables that may counteract the biochemical processes leading to onset of CVDs and other NCDs [39]. Equally dissimilar vegetable categories differ in nutritional composition, the associations with wellness outcomes may differ as well [39].
Although the health benefits of fruits and vegetables are ordinarily studied together in most studies [1,11,13,xv,16,23,25,32,34], it is recommended that the benefits of these ii nutrient groups are assessed separately. Fruits and vegetables share wellness benefits due to mutual phytochemicals (east.chiliad., phenolics, flavonoids, carotenoids), vitamins (e.thousand., vitamin C, folate, pro-vitamin A), minerals (east.one thousand., potassium, calcium, magnesium) and fibers, but bioactive compounds differ widely in composition and ratio between fruits and vegetables [40,41,42,43]. Moreover, fruits accept ordinarily a college concentration of sugars than vegetables, while vegetables are more probable to have a college concentration of fibers and proteins [40]. Particularly when fruit juices are included in fruit measurements, benign furnishings of fruits alone or in combination with vegetables may not get apparent due to higher intakes in sugar and free energy from fruit juices [44]. In fact, studies that have separated fruit and vegetable groups have shown differences in health outcomes [vi,22,24,36,38,40,45,46,47]. For instance, in a written report by Villegas et al. (2008), the increased intake of specific vegetable groups was significantly inversely associated with the blazon 2 diabetes risk, while this clan was not plant for increased fruit intake in Chinese women [24].
According to World Wellness Organization (WHO) and Food and Agronomics Organization (FAO) guidelines (2003), the recommended consumption of fruits and vegetables is at to the lowest degree 400 g/day [48]. While it is generally believed that vegetable intake is inadequate in most countries [49,50,51,52], at that place is currently no systematic review that focuses solely on vegetable intake to confirm these assumptions. The Global Burden of Disease (GBD) Study 2010 assessed vegetable intake and concluded that the intake was mostly too low to minimize the hazard of chronic diseases [49,l]. However, in this study vegetable intake was combined with that of legumes and not all information included was assessed at the individual level. Hall et al. (2009) [52] ended that low vegetable and fruit consumption is higher in depression- and eye-income countries, but did not carve up fruit and vegetable intake.
Therefore, the main aim of the current report is to systematically review the vegetable consumption in developed populations of xviii years and older globally and to compare these information to the existing recommendations and to vegetable supply data.
2. Materials and Methods
2.1. Definitions
The definition of "vegetables" varies significantly among different countries and regions and consequently local recommendations on vegetable intake differ. In the current review, the definition for "vegetables" past WHO/FAO is followed, which excludes potatoes, tubers, legumes and pulses [53].
We derived a vegetable intake recommendation from the global recommendation by FAO/WHO (2003) of ≥400 g/solar day (v servings of 80 g) for fruit and vegetables, every bit there is no specific guideline for vegetables alone [48]. Every bit nearly countries follow the FAO/WHO guidelines and the majority suggest that at least three servings (240g/day) should come up from vegetables [54,55], we set the vegetable intake recommendation at ≥240 one thousand/day.
2.2. Search Strategy
The search was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines from March 2018 to June 2019 (meet Supplementary Materials, Table S1) [56]. Data about vegetable intake was preferably taken from national nutrition surveys in social club to excerpt the most representative vegetable intake data. Therefore, we beginning searched these surveys per country from government websites and online databases from health authorities [57,58]. The European Food Safety Authority (EFSA) Comprehensive European Food Consumption Database was used every bit a guide for reviewing the existing national nutrition surveys in Europe [59]. For some European countries for which the national survey reports did not report vegetable intake separately from potatoes and legumes, vegetable intake data was taken from the EFSA database. The STEPwise approach to surveillance (STEPS) database was also consulted for available vegetable intake data. STEPS is a simple, standardized method for collecting, analyzing and disseminating information regarding surveillance of NCD hazard factors, with a non-itemized Nutrient Frequency Questionnaire (FFQ) on vegetable intake. STEPS surveys are usually initiated and conducted by Ministry of Health officials in collaboration with local technical partners [4].
When for a country no nationally representative survey with relevant vegetable intake data was retrieved, a literature search in PubMed was conducted. The search string was a combination of the following terms: "dietary intake" OR "food consumption" OR "vegetable intake" OR "vegetable consumption" AND "land name". There were no language restrictions in the overall search. Papers were screened and selected co-ordinate to titles and abstracts, followed past a full-text review for final inclusion, using the following inclusion criteria:
-
Information from adult populations aged ≥18 years.
-
Costless living, healthy population. Disabled people, populations with specific diseases or with special dietary needs (pregnant and lactating women, athletes) were excluded.
-
National or population-based surveys/studies. In example these were not available, baseline data or data from a command group, belonging to a healthy full general population, of controlled trials were included.
-
Surveys/Studies conducted from the year 2000 onwards and published until June 2019.
-
Sample size of participants ≥100.
-
Surveys/Studies in which vegetable intake in adults at individual level were included (therefore, studies estimating vegetable intake per capita or at household level were excluded)
-
Countries and continent regions included were derived from the UN Geoscheme created by United nations Statistics Division and World Atlas [57,58].
2.3. Data Extraction
Data extraction was conducted by two independent researchers to eliminate information extraction errors. Means and 95% confidence intervals (95% CI) were mainly extracted; if not available, medians, Standard Deviations (SD), percentiles, ranges, and Standard Errors (SE) were extracted. Additionally, data about gender, age, sample size, yr of survey conduct, year of publication, report blazon, sample representativeness and vegetable intake assessment methodology were extracted.
2.4. Quality Assessment of the Data
Representativeness was divers in 3 levels. A sample was considered highly representative when: 1) there was a statement by the authors of the survey/written report that the sample was representative for the target population, simply likewise covered all or nearly of the regions of a country; ii) its representativeness was addressed by the methodology used and the stratification of the sample (distribution of sample according to historic period, gender, education, regions etc.). A sample was considered moderately representative when at to the lowest degree one of the higher up criteria was followed, but participants from most of the country's regions were not included. A sample was not considered representative when none of the representativeness criteria were met [60].
2.5. Data Analysis
Vegetable consumption was expressed in grams per day. Descriptive statistics were used for the analysis of vegetable intake. For six countries for which no data on vegetable consumption alone were plant, nosotros used data where vegetable and fruit intake were reported together and causeless that vegetable consumption covered lx% of the intake co-ordinate to WHO/FAO recommendation almost vegetable and fruit intake. When ways and 95% CIs were expressed for subgroups of gender, age or ethnicity, a weighted mean and 95% CI were calculated using the mean, 95% CI and the number of participants of each group. When data were not expressed in means and 95% CIs, then data were converted using the following equations.
-
For the conversion of medians and ranges into ways [61]:
where
= mean, a = minimum, b = maximum and 1000 = median.
- 2.
-
For conversion of median and 25th and 75th percentiles into ways [62]:
where
= hateful, q1 = P25, m = median, q3 = P75.
- three.
-
For mean and SE into 95% CIs [63]:
- 4.
-
For mean and SD into 95% CIs [63]:
- five.
-
For 25th and 75th percentiles into 95% CI [62], first a conversion was fabricated into SD and then into 95% CI following the equation in a higher place (four):
- half-dozen.
-
For 5th and 95th into 95% CI [62], first a conversion was made into SD then into 95% CI post-obit the equation to a higher place (4):
For each region, we calculated a weighted mean vegetable intake where nosotros used the adult population of xviii years and older in 2013 every bit derived from United Nations Children's Fund (UNICEF) Land of the World's Children report, 2015 [64].
2.vi. Vegetable Supply Data
Vegetable supply per country was extracted and calculated according to data from the well-nigh recent food balance sheets by Food and Agronomics Organization Corporate Statistical Database (FAOSTAT) (2013) [65]. The vegetable supply was the sum of the supply information from the food categories onions, tomatoes and their products, peas and other vegetables: and excluded legumes, potatoes, tubers and pulses [65]. Vegetable supply was converted from kg/year/capita to 1000/24-hour interval/capita in guild to compare results with the vegetable intake information. For each region, nosotros calculated a weighted mean vegetable supply where we used the adult population in 2013 every bit weighing factor.
3. Results
3.i. Data Availability, Representativeness and Dietary Cess Methodology
The systematic search yielded initially 3247 publications (Figure ane). Later abstract and championship screening, 558 publications were assessed for eligibility. The final review dataset included 160 publications with studies measuring vegetable intake in 162 out of 235 countries, covering 93% of the world's adult population. Vegetable supply data were available for 136 out of the 162 (84%) countries with vegetable intake data; for the smaller countries vegetable supply information was more often than not lacking.
The surveys/studies included in this review had a high sample representativeness, with only 28 (17%) with a non-representative sample and six (4%) with no information about sample representativeness (run across Supplementary Materials, Tabular array S2). The sample size of the surveys/studies ranged from 100 subjects in Jamaica to 140,859 in Mainland china.
The most frequently used method to appraise vegetable intake was a (semi-) quantitative FFQ (65%), which also includes the STEPS methodology which was used in most African, Latin American and Oceanian countries. Vegetable intake data in high-income countries were more often than not from national nutrition surveys in which a combination of 24 h dietary recalls and FFQs were used (come across Supplementary Materials, Table S2).
3.2. Global Vegetable Intake and Supply
Based on data of 162 countries, the weighted mean vegetable intake was 186 g/day and ranged from 56 1000/day in Central America to 349 g/day in Eastern asia (Tabular array 1). Based on information from 136 countries, the weighted mean global vegetable supply was 431 g/day and ranged widely among the different regions from 71 g/mean solar day in Melanesia to 882 thousand/day in East asia. Details of vegetable intake and supply per land can exist establish in the supporting information, Tabular array S2. Asia was the continent with the highest vegetable consumption, where 10 countries (29%) met the recommendations, while in Oceania 2 (11%), Africa three (7%), Europe 4 (11%) and America i (7%) countries had an adequate consumption of vegetables (Table 1). In Europe, 26 out of 36 (72%) and in Asia, 19 out of 31 countries (61%) had an adequate vegetable supply to meet the vegetable recommendation of ≥240 chiliad/day; whereas in Africa 5 out of 39 countries (13%) had a sufficient vegetable supply to meet the recommendation.
Figure 2 provides an overview of the vegetable intake and supply data against the vegetable recommendations of ≥240 g/day based on data of 136 countries. Just 10 out of 136 countries (7%) have an acceptable intake and adequate supply of vegetables, whereas in 119 of the 136 countries (88%) vegetable intake is below the recommendations. Moreover, in 73 of these 119 countries (61%) vegetable supply is inadequate to run into the recommendations. For seven countries, vegetable intake was adequate, but vegetable supply information were below 240 grand/mean solar day.
3.three. Asia
Vegetable intake data was absent for Key Asia. Among the other Asian regions, weighted mean vegetable intake ranged from 81 g/mean solar day (mean lowest and highest intake in region countries: 56, 304 g/solar day) in Southern asia to 349 (80, 357) g/day in Due east Asia. In East Asia four out of six countries (67%) met the recommendations for vegetable intake, whereas this was the case for ix–29% of the countries in the other Asian regions (Table ane). The weighted mean vegetable supply ranged widely within and amidst the Asian regions; from 190 (92, 577) thou/twenty-four hours in S East Asia to 882 (149, 969) g/24-hour interval in E Asia. But in South E Asia the weighted mean vegetable supply was below 240 chiliad/24-hour interval, whereas that of Southern asia was just above the recommendations with 264 g/24-hour interval.
3.4. Europe
Vegetable intake data was available for 37 out of 56 European countries and in iv Due north European countries (Republic of iceland, Denmark, Norway, Lithuania) legumes were included in the vegetable intake measurements. Weighted mean vegetable intake ranged from 123 (95, 207) 1000/solar day in Western Europe to 270 (83, 382) in Eastern Europe (Table 1). Out of 37 European countries, four countries met the vegetable intake recommendations of ≥240 g/day, including one in Southern and three countries in Eastern Europe. The weighted mean vegetable supply ranged from 269 (239, 379) 1000/24-hour interval in Western Europe to 453 (221, 662) chiliad/mean solar day in Southern Europe. In 10 out of 36 countries, the vegetable supply was not sufficient to run into the recommended intake of 240 g/solar day.
3.5. America
Vegetable intake data was available for 28 out of 54 countries in the Americas. Weighted mean vegetable intake ranged from 56 (1–88) m/day in Cardinal America to 156 (48, 263) grand/mean solar day in Northward America (Tabular array 1). Of all the American countries, one S American land met the recommendations for vegetable intake. The weighted hateful vegetable supply ranged from 102 (53, 252) g/day in the Caribbean area to 277 (153, 474) g/24-hour interval in North America. In Central and South America and the Caribbean the weighted hateful vegetable supply was below 240 g/day, whereas in three out of four North American countries the vegetable supply was just above the recommendations with 277 one thousand/mean solar day.
3.6. Oceania
Vegetable intake data was available for eighteen out of 32 countries in Oceania. Weighted mean vegetable intake ranged from 73 (64, 248) 1000/day in Melanesia to 196 (72, 417) g/day in Polynesia (Table 1). The vegetable intake met the recommendation in ii of the xviii countries. The weighted mean vegetable supply ranged from 71 (37, 142) yard/day in Melanesia to 295 (283, 357) g/day in Australasia. Only in Australasian countries the vegetable supply was higher up 240 g/day.
iii.7. Africa
Vegetable intake data was available for 44 out of 62 countries in Africa. The weighted hateful vegetable intake ranged from 98 (28, 304) g/24-hour interval in Eastward African countries to 135 (88, 168) g/solar day in South Africa (Table 1). In 3 out of the 44 African countries vegetable intake recommendations were met. The weighted hateful vegetable supply ranged from 86 (48, 206) one thousand/day in Due east African countries to 434 (230, 531) chiliad/day in N Africa. Only in North Africa was the weighted hateful vegetable supply sufficient to meet the recommendation of 240 g/solar day.
4. Discussion
Weighted hateful vegetable intake was 186 yard/day and ranged from 56 g/day in Central America to 349 g/solar day in East asia. Weighted mean vegetable supply was 431 g/day and ranged widely among the different regions from 71 g/day in Melanesia to 882 g/day in East Asia. For 88% of the countries, vegetable intake was below the recommendations and for 61% the vegetable supply was too low to meet the recommendations of 240 m/day.
To our knowledge this is the beginning systematic review evaluating global vegetable intake (excluding legume and potato intake) at an individual level with a comparison to vegetable recommendation and vegetable supply. For 82% of the surveys/studies that were identified, vegetable intake data was compliant with the vegetable definition of FAO/WHO [53]. For 4% of the countries where fruit and vegetable intake were reported together, we fabricated the supposition that sixty% of the intake would come from vegetables, which may have resulted in either over- or underestimation of the intake. Only the almost recent surveys of each state were selected, with 65% of the surveys/studies conducted in the terminal decade. Another important strength of this review is the high representativeness of the vegetable intake data, since for nearly lxxx% of the countries included the data extracted was nationally representative.
Limitations of our review with regard to the vegetable intake data are mainly due to heterogeneity among studies, including differences in the methods of assessing vegetable intake, differences in the definition of vegetable intake and differences in the units of reporting. For dietary intake of vegetables, the most common method was a (semi-)quantitative FFQ at individual level, which was used in 65% of the identified surveys/studies. A recent review on dietary intake measurements of vegetable and fruits in Europe, indicated also that FFQs were more often than not used [3]. This review indicated that FFQs may differ in a number of aspects, such as (not)-itemization of terms, inclusion of potatoes and legumes in vegetable definition, and portion size adding. This may likewise explicate part of the variation in vegetable consumption between studies in our review. For instance, in many of the studies included in our review it was unclear whether soups, vegetable juices, processed vegetables and mixed dishes containing vegetables were included and hence vegetable intake may be underestimated. Furthermore, we noticed heterogeneity in calculation and reporting of vegetable intake information among the surveys that were using the STEPS methodology. Lastly, due to heterogeneity in reporting units, it was not possible to convert all data to means and SDs and hence it was non possible to calculate the prevalence of inadequate vegetable intake per country and region. Therefore, nosotros decided to report vegetable intake in ways and 95% CI.
Vegetable supply data may exist underestimated as the information from FAO Food Balance Sheets are reported per capita and therefore comprise information for the entire population, including children. Furthermore, exclusion of vegetables that are cropped privately or in the wild [53,66] and unavailability of production data of all regions within a country [66] in Food Balance Canvass data may have led to underestimation of vegetable supply. These limitations may partly explain the finding that for some countries the vegetable supply was lower than the intake. Other reasons for this finding can be attributed to limitations of the studies' measuring of vegetable intake, e.thou., non-representativeness of intake data, lack of addressing seasonal differences in vegetable intake, and large differences between the year that the intake data were collected and the twelvemonth of the supply information.
Our finding that vegetable intake worldwide is low (186 g/twenty-four hour period) with many low- and centre-income countries in the range of one–2 portions per 24-hour interval, correspond with that of earlier reviews. The GBD study of 2010 reported a mean intake of 209 g/day including legumes and starchy vegetables [49,l]. Similarly, the Prospective Urban Rural Epidemiology (PURE) study [51] and World Health Survey 2002–2003 [52] indicated that fruit and vegetable intake were below the recommendations and the intakes were generally lower in low- and middle income countries. I of the main reasons for the depression vegetable intake in the low- and middle-income countries is urbanization and shift to a more "western" diet, high in foods that are high in sugar, fatty, and salt and low in fiber. In add-on, in these countries in that location is generally a lack of secure availability and affordability of vegetables, which are underlying causes for an inadequate intake of vegetables [51].
An of import finding of our review is that even though the weighted vegetable supply worldwide is sufficient (431 k/solar day), vegetable supply among the countries varies widely and consequently in many countries it is insufficient to adhere to the recommended intake of 240 grand/twenty-four hours. With a shift to a more found-based nutrition, as recently recommended by the Eat-Lancet commission, vegetable intake recommendations are further increasing to 300 thou/day [67]. This would imply that in the vast majority (93%) of the countries globally, vegetable supply would not be sufficient. The Eat-Lancet committee predicts that an increase of 75% in product of vegetables is needed together with accompanying measures to prevent losses in vegetable supply, e.g., preservation techniques such as drying, canning and freezing of vegetables. Moreover, improvements in the infrastructure are needed to facilitate the distribution of vegetables and innovative approaches to improve accessibility of fresh vegetables to consumers are essential to improve vegetable consumption.
To further improve vegetable intake, consumers should be educated about the benefits of vegetables for health. International recommendations should go more specific concerning the categories included and the portion sizes of raw and cooked vegetables. The development of country specific food based dietary guidelines including a recommendation for vegetable intake tin can play a part in this, although many countries have not nevertheless developed these or the recommendation is unclear [68]. Later, the national nutrition policy makers could develop detailed guidelines which are in line with the international guidelines by WHO/FAO and translated to the dietary goals and traditions of the country. These guidelines should include practical examples of traditional cooking methods and recipes to increase vegetable intake. Moreover, community-based activities like community kitchens could be organized [69]. The objective would be to educate the populations about healthy dietary patterns according to national dietary guidelines, including the importance of vegetables and vegetable categories, and to improve cooking and purchasing skills adjusted to the national and regional culture. While the effectiveness of public wellness interventions to increase vegetable intake through education and counseling is mostly positive, unclarity exists most whether the achievements remain in the longer term [seventy,71,72]. In order to modify the behavior of the consumer, it is important that the environment should be encouraging and rewarding. Besides an adequate supply and accessibility, affordability of vegetables is key. The PURE study (2016) indicated that low income countries spend a college percentage of the households' income on vegetables compared to high income countries [51]. Governments need to play a role to ensure that vegetables become affordable to the entire population, including the lower income consumers. A modelling study estimated that, even under optimistic socioeconomic scenarios with economic growth, the future supply of vegetables will be bereft to come across the recommendations for many countries [73]. This prediction makes even more imperative the need to tackle the global problem of nutrient loss and waste, especially in the case of vegetables that are considered sensitive nutrient products and whose loss can easily occur due to poor practices and degradation [74]. Nevertheless, locally grown and sourced vegetables, and inclusion of indigenous vegetables may assist to ensure a fresh and sustainable vegetable supply. Furthermore, learning from public wellness strategies aimed at increasing vegetable intake in the countries with an adequate vegetable intake should be taken into account.
Lastly, it would exist beneficial to get a better agreement of the health properties of the different vegetables and how different processing techniques will influence the effect of vegetables on health. This could pb to more detailed guidance on vegetable consumption; for case, in the German guidelines, specific recommendations were provided for raw and cooked vegetables. In society to monitor whether populations adhere to the guidelines and to let for land comparisons, harmonization of the methodology used to collect vegetable intake data, including standard dietary methods and measurement units, is recommended.
five. Conclusions
In determination, our review indicated that global vegetable intake is generally below the recommendations of 240 m/day and that the vegetable supply is generally inadequate to meet the recommendations. With the current emphasis on consuming institute-based diets, efforts are needed to improve the production, accessibility and affordability of vegetables in conjunction with innovative approaches to found a sustained behavior alter aimed at improving vegetable intake worldwide.
Supplementary Materials
The following are available online at https://www.mdpi.com/2072-6643/12/6/1558/s1, Table S1: PRISMA checklist, Tabular array S2: Vegetable intake, socio-demographics, sample size and representativeness, vegetable intake data source and dietary method used per country.
Author Contributions
Conceptualization, A.1000., A.Due east. and E.T.; methodology, A.K., A.East. and E.F.T.; formal assay, A.K.; investigation, A.K.; data curation, A.K. and A.E.; writing—original draft preparation, A.K. and A.E.; writing—review and editing, A.E., A.K. and Due east.F.T.; visualization, A.K.; supervision, A.Thousand. and E.F.T. All authors take read and agreed to the published version of the manuscript.
Funding
This research was partly conducted every bit internship projection of A.G., which was funded by Unilever. The APC was funded by Wageningen Academy and Inquiry.
Conflicts of Involvement
A.E. is employee of Unilever. The other authors do not have a conflict of interest.
References
- Darfour-Oduro, S.A.; Buchner, D.G.; Andrade, J.E.; Grigsby-Toussaint, D.S. A comparative written report of fruit and vegetable consumption and physical activity among adolescents in 49 Low-and-Middle-Income Countries. Sci. Rep. 2018, 8, 1623. [Google Scholar] [CrossRef]
- Diet, diet and the prevention of chronic diseases. Earth Health Organ. Tech. Rep. Ser. 2003, 916. i–8, 1–149, backcover.
- Riordan, F.; Ryan, K.; Perry, I.J.; Schulze, M.B.; Andersen, Fifty.F.; Geelen, A.; Van't Veer, P.; Eussen, South.; Dagnelie, P.; Wijckmans-Duysens, N.; et al. A systematic review of methods to assess intake of fruits and vegetables among healthy European adults and children: A DEDIPAC (DEterminants of Diet and Physical Activity) study. Public Wellness Nutr. 2017, 20, 417–448. [Google Scholar] [CrossRef] [PubMed]
- Riley, Fifty.; Guthold, R.; Cowan, M.; Savin, S.; Bhatti, L.; Armstrong, T.; Bonita, R. The Globe Health Arrangement STEPwise Approach to Noncommunicable Disease Risk-Factor Surveillance: Methods, Challenges, and Opportunities. Am. J. Public Health 2016, 106, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Wellness Arrangement, W. Global Health Risks. Mortality and Burden Och Illness Attributable to Selected Major Risks; Wellness System: Geneva, Switzerland, 2009; pp. ane–63. [Google Scholar]
- Dauchet, L.; Amouyel, P.; Hercberg, Due south.; Dallongeville, J. Fruit and vegetable consumption and chance of coronary heart disease: A meta-assay of cohort studies. J. Nutr. 2006, 136, 2588–2593. [Google Scholar] [CrossRef]
- Joshipura, Chiliad.J.; Hu, F.B.; Manson, J.Due east.; Stampfer, M.J.; Rimm, Eastward.B.; Speizer, F.E.; Colditz, G.; Ascherio, A.; Rosner, B.; Spiegelman, D.; et al. The consequence of fruit and vegetable intake on risk for coronary heart disease. Ann. Intern. Med. 2001, 134, 1106–1114. [Google Scholar] [CrossRef]
- Oyebode, O.; Gordon-Dseagu, Five.; Walker, A.; Mindell, J.S. Fruit and vegetable consumption and all-cause, cancer and CVD mortality: Analysis of Health Survey for England data. J. Epidemiol. Commun. Wellness 2014, 68, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Lock, K.; Pomerleau, J.; Causer, L.; Altmann, D.R.; McKee, M. The global brunt of disease owing to low consumption of fruit and vegetables: Implications for the global strategy on nutrition. Balderdash Globe Wellness Organ 2005, 83, 100–108. [Google Scholar]
- He, F.J.; Nowson, C.A.; Lucas, M.; MacGregor, G.A. Increased consumption of fruit and vegetables is related to a reduced risk of coronary heart disease: Meta-analysis of cohort studies. J. Hum. Hypertens. 2007, 21, 717. [Google Scholar] [CrossRef]
- He, F.J.; Nowson, C.A.; MacGregor, G.A. Fruit and vegetable consumption and stroke: Meta-assay of cohort studies. Lancet 2006, 367, 320–326. [Google Scholar] [CrossRef]
- Hu, D.; Huang, J.; Wang, Y.; Zhang, D.; Qu, Y. Fruits and Vegetables Consumption and Risk of Stroke. Meta-Anal. Prospect. Cohort Stud. 2014, 45, 1613–1619. [Google Scholar] [CrossRef]
- Crowe, F.; Westward Roddam, A.; J Key, T.; Northward Appleby, P.; Overvad, G.; Jakobsen, Yard.; Tjønneland, A.; Hansen, L.; Boeing, H.; Weikert, C.; et al. Fruit and Vegetable Intake and Mortality from Ischaemic Center Disease: Results from the European Prospective Investigation into Cancer and Nutrition (Ballsy)-Heart Study. Eur. Heart J. 2011, 32, 1235–1243. [Google Scholar] [CrossRef] [PubMed]
- Borgi, L.; Muraki, I.; Satija, A.; Willett, W.C.; Rimm, Due east.B.; Forman, J.P. Fruit and Vegetable Consumption and the Incidence of Hypertension in Three Prospective Cohort Studies. Hypertension 2016, 67, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Li, F.; Wang, L.; Zhang, D. Fruit and Vegetables Consumption and Risk of Hypertension: A Meta-Analysis. J. Clin. Hypertens. (Greenwich Conn,) 2016, 18, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Bhupathiraju, Southward.N.; Wedick, N.M.; Pan, A.; Manson, J.Due east.; Rexrode, K.Thou.; Willett, Westward.C.; Rimm, East.B.; Hu, F.B. Quantity and variety in fruit and vegetable intake and risk of coronary heart illness. Am. J. Clin. Nutr. 2013, 98, 1514–1523. [Google Scholar] [CrossRef]
- Dauchet, 50.; Amouyel, P.; Dallongeville, J. Fruit and vegetable consumption and risk of stroke: A meta-analysis of accomplice studies. Neurology 2005, 65, 1193–1197. [Google Scholar] [CrossRef]
- Zhan, J.; Liu, Y.J.; Cai, Fifty.B.; Xu, F.R.; Xie, T.; He, Q.Q. Fruit and vegetable consumption and risk of cardiovascular disease: A meta-analysis of prospective cohort studies. Crit. Rev. Food Sci. Nutr. 2017, 57, 1650–1663. [Google Scholar] [CrossRef]
- Kaiser, K.A.; Brown, A.W.; Bohan Brown, M.Chiliad.; Shikany, J.One thousand.; Mattes, R.D.; Allison, D.B. Increased fruit and vegetable intake has no discernible consequence on weight loss: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2014, 100, 567–576. [Google Scholar] [CrossRef]
- Tapsell, L.C.; Dunning, A.; Warensjo, Due east.; Lyons-Wall, P.; Dehlsen, K. Furnishings of vegetable consumption on weight loss: A review of the evidence with implications for design of randomized controlled trials. Am. J. Clin. Nutr. 2014, 54, 1529–1538. [Google Scholar] [CrossRef]
- Ledoux, T.A.; Hingle, M.D.; Baranowski, T. Relationship of fruit and vegetable intake with adiposity: A systematic review. Obes. Rev. 2011, 12, e143–e150. [Google Scholar] [CrossRef]
- Carter, P.; Gray, L.J.; Troughton, J.; Khunti, Thousand.; Davies, Thou.J. Fruit and vegetable intake and incidence of blazon two diabetes mellitus: Systematic review and meta-analysis. BMJ (Clin. res. ed.) 2010, 341. [Google Scholar] [CrossRef]
- Harding, A.H.; Wareham, N.J.; Bingham, S.A.; Khaw, K.; Luben, R.; Welch, A.; Forouhi, North.1000. Plasma vitamin C level, fruit and vegetable consumption, and the risk of new-onset type two diabetes mellitus: The European prospective investigation of cancer--Norfolk prospective study. Curvation. Intern. Med. 2008, 168, 1493–1499. [Google Scholar] [CrossRef] [PubMed]
- Villegas, R.; Shu, X.O.; Gao, Y.T.; Yang, G.; Elasy, T.; Li, H.; Zheng, W. Vegetable but not fruit consumption reduces the chance of type 2 diabetes in Chinese women. J. Nutr. 2008, 138, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Bazzano, L.A.; Li, T.Y.; Joshipura, M.J.; Hu, F.B. Intake of fruit, vegetables, and fruit juices and gamble of diabetes in women. Diabetes Intendance 2008, 31, 1311–1317. [Google Scholar] [CrossRef] [PubMed]
- Montonen, J.; Jarvinen, R.; Heliovaara, M.; Reunanen, A.; Aromaa, A.; Knekt, P. Food consumption and the incidence of blazon Two diabetes mellitus. Eur. J. Clin. Nutr. 2005, 59, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Serdula, M.; Janket, S.J.; Melt, North.R.; Sesso, H.D.; Willett, Due west.C.; Manson, J.E.; Buring, J.Due east. A prospective study of fruit and vegetable intake and the risk of type two diabetes in women. Diabetes Care 2004, 27, 2993–2996. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Mokdad, A.H. Fruit and vegetable consumption and diabetes mellitus incidence among U.S. adults. Prev. Med. 2001, 32, 33–39. [Google Scholar] [CrossRef]
- Meyer, K.A.; Kushi, L.H.; Jacobs, D.R., Jr.; Slavin, J.; Sellers, T.A.; Folsom, A.R. Carbohydrates, dietary fiber, and incident blazon 2 diabetes in older women. J. Clin. Nutr. 2000, 71, 921–930. [Google Scholar] [CrossRef]
- Hirayama, F.; Lee, A.H.; Binns, C.W.; Zhao, Y.; Hiramatsu, T.; Tanikawa, Y.; Nishimura, Chiliad.; Taniguchi, H. Do vegetables and fruits reduce the risk of chronic obstructive pulmonary disease? A case–control written report in Japan. Prev. Med. 2009, 49, 184–189. [Google Scholar] [CrossRef]
- Hosseini, B.; Berthon, B.Southward.; Wark, P.; Wood, L.G. Furnishings of Fruit and Vegetable Consumption on Risk of Asthma, Wheezing and Immune Responses: A Systematic Review and Meta-Analysis. Nutrients 2017, 9. [Google Scholar] [CrossRef]
- Soerjomataram, I.; Oomen, D.; Lemmens, V.; Oenema, A.; Benetou, V.; Trichopoulou, A.; Coebergh, J.W.; Barendregt, J.; de Vries, Eastward. Increased consumption of fruit and vegetables and future cancer incidence in selected European countries. Eur. J. Cancer 2010, 46, 2563–2580. [Google Scholar] [CrossRef] [PubMed]
- Leenders, Thousand.; Siersema, P.D.; Overvad, K.; Tjonneland, A.; Olsen, A.; Boutron-Ruault, M.C.; Bastide, N.; Fagherazzi, K.; Katzke, V.; Kuhn, T.; et al. Subtypes of fruit and vegetables, multifariousness in consumption and chance of colon and rectal cancer in the European Prospective Investigation into Cancer and Nutrition. Int. J. Cancer 2015, 137, 2705–2714. [Google Scholar] [CrossRef] [PubMed]
- Benetou, V.; Orfanos, P.; Lagiou, P.; Trichopoulos, D.; Boffetta, P.; Trichopoulou, A. Vegetables and fruits in relation to cancer take a chance: Evidence from the Greek EPIC cohort report. Cancer Epidemiol. Biomark. Prev. 2008, 17, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Linseisen, J.; Rohrmann, S.; Miller, A.B.; Bueno-de-Mesquita, H.B.; Buchner, F.L.; Vineis, P.; Agudo, A.; Gram, I.T.; Janson, 50.; Krogh, V.; et al. Fruit and vegetable consumption and lung cancer risk: Updated data from the European Prospective Investigation into Cancer and Nutrition (Ballsy). Int. J. Cancer 2007, 121, 1103–1114. [Google Scholar] [CrossRef]
- Gonzalez, C.A.; Pera, M.; Agudo, A.; Bueno-de-Mesquita, H.B.; Ceroti, M.; Boeing, H.; Schulz, Grand.; Del Giudice, G.; Plebani, Yard.; Carneiro, F.; et al. Fruit and vegetable intake and the risk of stomach and oesophagus adenocarcinoma in the European Prospective Investigation into Cancer and Diet (Epic-EURGAST). Int. J. Cancer 2006, 118, 2559–2566. [Google Scholar] [CrossRef]
- Takachi, R.; Inoue, M.; Sugawara, Y.; Tsuji, I.; Tsugane, S.; Ito, H.; Matsuo, G.; Tanaka, Yard.; Tamakoshi, A.; Mizoue, T.; et al. Fruit and vegetable intake and the gamble of overall cancer in Japanese: A pooled analysis of population-based cohort studies. J. Epidemiol. 2017, 27, 152–162. [Google Scholar] [CrossRef]
- Wang, M.; Qin, S.; Zhang, T.; Song, Ten.; Zhang, Due south. The effect of fruit and vegetable intake on the evolution of lung cancer: A meta-analysis of 32 publications and xx 414 cases. Eur. J. Clin. Nutr. 2015, 69, 1184. [Google Scholar] [CrossRef]
- Li, G.; Fan, Y.; Zhang, Ten.; Hou, West.; Tang, Z. Fruit and vegetable intake and risk of blazon two diabetes mellitus: Meta-analysis of prospective cohort studies. BMJ Open 2014, 4, e005497. [Google Scholar] [CrossRef]
- Appleton, K.M.; Hemingway, A.; Saulais, 50.; Dinnella, C.; Monteleone, E.; Depezay, Fifty.; Morizet, D.; Armando Perez-Cueto, F.J.; Bevan, A.; Hartwell, H. Increasing vegetable intakes: Rationale and systematic review of published interventions. Eur. J. Nutr. 2016, 55, 869–896. [Google Scholar] [CrossRef]
- Liu, R.H. Health-promoting components of fruits and vegetables in the diet. Adv. Nutr. 2013, 4, 384S–392S. [Google Scholar] [CrossRef]
- Slavin, J.L.; Lloyd, B. Health Benefits of Fruits and Vegetables. Adv. Nutr. 2012, 3, 506–516. [Google Scholar] [CrossRef] [PubMed]
- Sharma, South.; Sheehy, T.; Kolonel, 50. Sources of vegetables, fruits, and vitamins A, C and Due east among five indigenous groups: Results from the Multiethnic Cohort Study. Eur. J. Clin. Nutr. 2014, 68, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Flood-Obbagy, J.E.; Rolls, B.J. The effect of fruit in dissimilar forms on energy intake and satiety at a repast. Appetite 2009, 52, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Van Duyn, M.A.S.; Pivonka, Due east. Overview of the Health Benefits of Fruit and Vegetable Consumption for the Dietetics Professional: Selected Literature. J. Am. Diet. Assoc. 2000, 100, 1511–1521. [Google Scholar] [CrossRef]
- Pem, D.; Jeewon, R. Fruit and Vegetable Intake: Benefits and Progress of Nutrition Education Interventions- Narrative Review Article. Iran. J. Public Health 2015, 44, 1309–1321. [Google Scholar] [PubMed]
- Loef, Yard.; Walach, H. Fruit, vegetables and prevention of cerebral turn down or dementia: A systematic review of accomplice studies. J. Nutr. Health Aging 2012, sixteen, 626–630. [Google Scholar]
- World Health Organization. Food and Agriculture Organization of the United Nations. Diet, Nutrition, and the Prevention of Chronic Diseases: Written report of a Joint WHO/FAO Good Consultation; Globe Health Organization: Geneva, Switzerland, 2003; p. 149. [Google Scholar]
- Micha, R.; Khatibzadeh, S.; Shi, P.; Andrews, K.Thousand.; Engell, R.Eastward.; Mozaffarian, D. Global, regional and national consumption of major food groups in 1990 and 2010: A systematic analysis including 266 country-specific nutrition surveys worldwide. BMJ Open 2015, v. [Google Scholar] [CrossRef]
- Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Illness Report 2016. Lancet 2017, 390, 1211–1259. [CrossRef]
- Miller, V.; Yusuf, S.; Chow, C.Thou.; Dehghan, M.; Corsi, D.J.; Lock, K.; Popkin, B.; Rangarajan, S.; Khatib, R.; Lear, Southward.A.; et al. Availability, affordability, and consumption of fruits and vegetables in 18 countries across income levels: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet Glob. Wellness 2016, four, e695–e703. [Google Scholar] [CrossRef]
- Hall, J.North.; Moore, S.; Harper, S.B.; Lynch, J.W. Global variability in fruit and vegetable consumption. Am. J. Prev. Med. 2009, 36, 402–409. [Google Scholar] [CrossRef]
- Agudo, A. Measuring Intake of fruit and Vegetables [electronic resource] / Antonio Agudo; World Health Organization: Geneva, Switzerland.
- Food-Based Dietary Guidelines. Available online: http://world wide web.fao.org/nutrition/education/nutrient-dietary-guidelines/home/en/ (accessed on fifteen March 2018).
- Inquiry, Westward.C.R.F.A.I.f.C. Nutrient, Diet, Physical Activeness, and the Prevention of Cancer: A Global Perspective; American Plant for Cancer Enquiry: Washington, DC, USA, 2007. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339. [Google Scholar] [CrossRef] [PubMed]
- Nag, O.S. The Regions Of Europe. thirteen March. Available online: https://www.worldatlas.com/articles/the-four-european-regions-as-defined-by-the-united-nations-geoscheme-for-europe.html (accessed on 13 March 2018).
- Sawe, B.E. What Is The United Nations Geoscheme? Available online: https://www.worldatlas.com/articles/what-is-the-united-nations-geoscheme.html (accessed on xiii March 2018).
- EFSA. The EFSA Comprehensive European Food Consumption Database. Available online: https://www.efsa.europa.eu/en/food-consumption/comprehensive-database (accessed on twenty June 2019).
- Hilger, J.; Friedel, A.; Herr, R.; Rausch, T.; Roos, F.; Wahl, D.A.; Pierroz, D.D.; Weber, P.; Hoffmann, K. A systematic review of vitamin D status in populations worldwide. Br. J. Nutr. 2014, 111, 23–45. [Google Scholar] [CrossRef] [PubMed]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, thirteen. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Barde, M.P.; Barde, P.J. What to employ to limited the variability of data: Standard deviation or standard error of mean? Perspect. Clin. Res. 2012, three, 113–116. [Google Scholar] [CrossRef] [PubMed]
- (UNICEF), U.N.C.s.F. The State of the World's Children 2015: Executive Summary. Reimagine the Future. Innovation for Every Child; UNICEF: New York, NY, U.s., 2014. [Google Scholar]
- Nutrient Residue Sheets. Available online: http://www.fao.org/economic/ess/fbs/en/ (accessed on 15 July 2019).
- Introduction. In Food Residue Sheets- A Handbook; FAO (Ed.) FAO: Rome, Italia, 2001. [Google Scholar]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, G.; Lang, T.; Vermeulen, Due south.; Garnett, T.; Tilman, D.; DeClerck, F.; Forest, A.; et al. Food in the Anthropocene: The Swallow–Lancet Commission on healthy diets from sustainable nutrient systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Herforth, A.; Arimond, One thousand.; Alvarez-Sanchez, C.; Coates, J.; Christianson, K.; Muehlhoff, E. A Global Review of Food-Based Dietary Guidelines. Adv. Nutr. 2019, ten, 590–605. [Google Scholar] [CrossRef]
- Plant of Medicine (US) and National Inquiry Council (The states) Committee on Babyhood Obesity Prevention Deportment for Local Governments. Actions for Salubrious Eating. In Local Government Actions to Prevent Childhood Obesity; Parker L, B.A., Sanchez, E., Eds.; National Academies Press (Usa): Washington, DC, U.s., 2009. [Google Scholar]
- Pomerleau, J.; Lock, Thousand.; Knai, C.; McKee, One thousand. Interventions designed to increment adult fruit and vegetable intake can exist effective: A systematic review of the literature. J. Nutr. 2005, 135, 2486–2495. [Google Scholar] [CrossRef]
- Conner, T.Southward.; Brookie, K.50.; Carr, A.C.; Mainvil, Fifty.A.; Vissers, M.C.M. Permit them eat fruit! The effect of fruit and vegetable consumption on psychological well-being in young adults: A randomized controlled trial. PLoS Ane 2017, 12, e0171206. [Google Scholar] [CrossRef]
- Plaete, J.; Crombez, 1000.; Van der Mispel, C.; Verloigne, M.; Van Stappen, V.; De Bourdeaudhuij, I. Result of the Web-Based Intervention MyPlan one.0 on Self-Reported Fruit and Vegetable Intake in Adults Who Visit Full general Do: A Quasi-Experimental Trial. J. Med. Internet Res. 2016, xviii, e47. [Google Scholar] [CrossRef]
- Mason-D'Croz, D.; Bogard, J.R.; Sulser, T.B.; Cenacchi, N.; Dunston, S.; Herrero, M.; Wiebe, K. Gaps between fruit and vegetable production, need, and recommended consumption at global and national levels: An integrated modelling study. Lancet. Planet. Wellness 2019, 3, e318–e329. [Google Scholar] [CrossRef]
- Ishangulyyev, R.; Kim, Due south.; Lee, South.H. Agreement Food Loss and Waste matter-Why Are We Losing and Wasting Food? Foods 2019, 8, 297. [Google Scholar] [CrossRef] [PubMed]
Figure 1. Flowchart of the review process for the selection of the final surveys/studies assessed.
Figure 1. Flowchart of the review process for the selection of the final surveys/studies assessed.
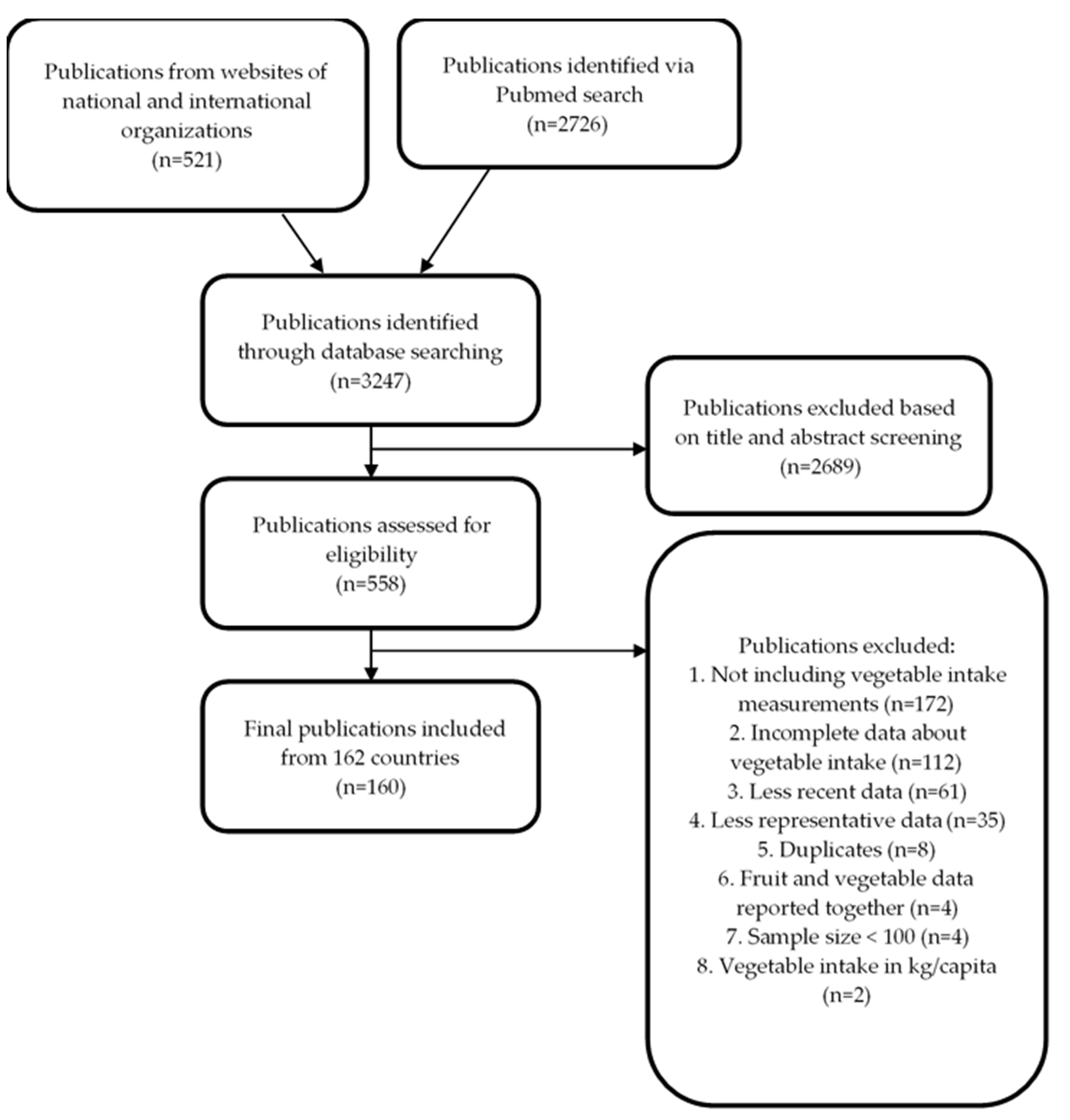
Figure 2. Vegetable intake and supply per country benchmarked against the vegetable recommendations of 240 g/day (WHO/FAO).
Figure 2. Vegetable intake and supply per country benchmarked against the vegetable recommendations of 240 thousand/mean solar day (WHO/FAO).
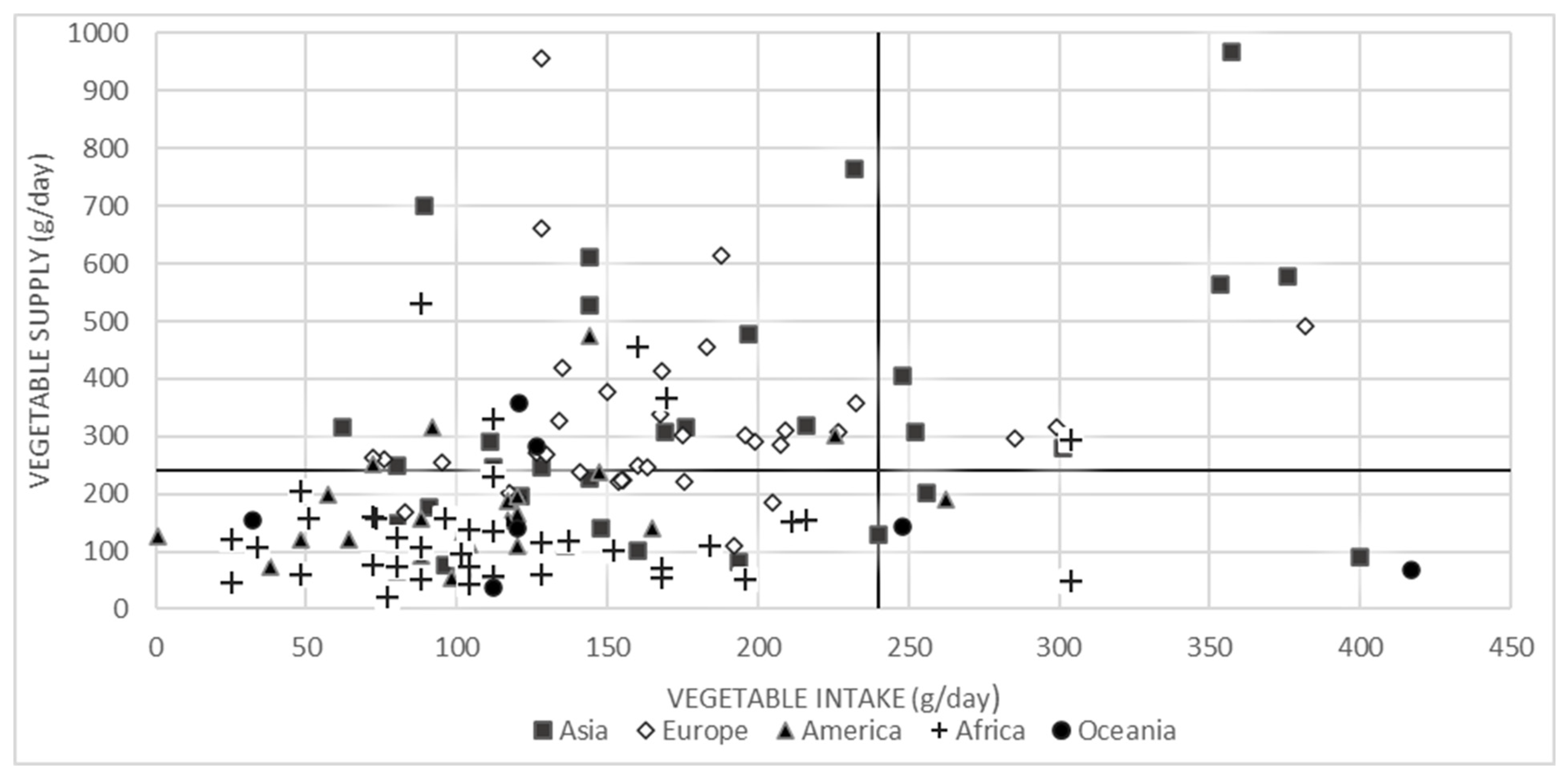
Table i. Vegetable intake expressed in average and range (g/d) and number (%) of countries co-ordinate to vegetable servings/d per continent region [57,58].
Table ane. Vegetable intake expressed in boilerplate and range (1000/d) and number (%) of countries according to vegetable servings/d per continent region [57,58].
| Continent | Region | Number of countries in the Region | Vegetable intake per Region (grand/twenty-four hour period) | Vegetable Supply per Region (thousand/solar day) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Countries with Information (n) | Weighted Mean | Range | Countries with Vegetable Intake ≥240 g/day (%) | Countries with Information (north) | Weighted Mean | Range | % of Vegetable Supply Consumed | |||
| Asia | West | 11 | eleven | 144 | 89–256 | 9 | 9 | 545 | 202–765 | 26 1 |
| Due east | 8 | 6 | 349 | lxxx–357 | 67 | vi | 882 | 149–969 | 40 1 | |
| Southeast | 13 | eleven | 153 | 91–400 | 27 | 10 | 190 | 92–577 | 80 four | |
| South | 8 | 7 | 81 | 62–304 | 29 | 6 | 264 | 75–315 | 31 three | |
| Europe | East | thirteen | 12 | 270 | 83–382 | 25 | 12 | 323 | 109–956 | 84 2 |
| North | 17 | ten | 132 | 72–227 | 0 | 10 | 270 | 192–339 | 49 | |
| South | 17 | 9 | 167 | 128–240 | 11 | 8 | 453 | 221–662 | 37 | |
| West | 9 | 6 | 123 | 95–207 | 0 | half dozen | 269 | 239–379 | 46 | |
| America | Central | seven | 2 | 56 | one–88 | 0 | 2 | 145 | 127–156 | 39 |
| Due south | 12 | 8 | 156 | 48–263 | xiii | 8 | 148 | 64–197 | 106 3 | |
| Caribbean | 29 | 14 | 104 | 38–163 | 0 | 9 | 102 | 53–252 | 102 i | |
| N | vi | iv | 108 | 92–226 | 0 | four | 277 | 153–474 | 39 | |
| Oceania | Australasia | 5 | 3 | 126 | 23–127 | 0 | 2 | 295 | 283–357 | 43 |
| Melanesia | 7 | 3 | 73 | 64–248 | 33 | 2 | 71 | 37–142 | 103 one | |
| Micronesia | viii | 5 | 122 | 32–216 | 0 | ane | 155 | 155–155 | 78 | |
| Polynesia | 12 | 7 | 196 | 72–417 | 14 | 2 | 110 | 67–140 | 178 1 | |
| Africa | N | xi | 5 | 122 | 88–170 | 0 | four | 434 | 230–531 | 28 |
| East | 20 | fourteen | 98 | 28–304 | 7 | 10 | 86 | 48–206 | 114 v | |
| Central | 9 | half dozen | 103 | 25–304 | 17 | six | 134 | 21–294 | 77 4 | |
| Due west | 17 | xiv | 123 | 25–216 | 7 | fourteen | 122 | 46–331 | 101 half-dozen | |
| South | 5 | 5 | 135 | 88–168 | 0 | 5 | 114 | 54–119 | 118 4 | |
© 2020 past the authors. Licensee MDPI, Basel, Switzerland. This article is an open access commodity distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Source: https://www.mdpi.com/2072-6643/12/6/1558/htm
{kind=link}
Post a Comment for "Increasing Vegetable Intakes Rationale and Systematic Review of Published Interventions"